Herniated Disc Bpc 157 Peptides for herniated disc: the complete recovery guide
Introduction
If you’ve been diagnosed with a herniated disc, you already know how stubborn the pain can be—sitting hurts, sleeping is disrupted, and even simple workouts feel risky. In my hands-on work with patients and clients navigating back pain, one question comes up constantly: “Can peptides help, and where does herniated disc bpc 157 fit into a safe recovery plan?”
This guide is a complete, practical recovery roadmap. I’ll explain how BPC-157 is discussed for disc-related injuries, what recovery stages look like, how to reduce the chance of setbacks, and which red flags mean you should escalate care. You’ll leave with a plan you can implement immediately—starting today.
Understanding a Herniated Disc (and Why Recovery Feels So Slow)
What’s actually happening
A herniated disc occurs when the soft inner material of a spinal disc pushes through a weak spot, potentially irritating nearby nerves. That irritation is often what drives the classic symptoms: radiating pain (sciatica), numbness/tingling, weakness, and sensitivity to certain movements or postures.
Why “healing the disc” isn’t a single event
In my experience, most people try to force recovery to happen on a calendar. But spinal recovery usually progresses through overlapping phases:
- Symptom calming: reduce nerve irritation and inflammatory flare-ups
- Tissue tolerance rebuilding: restore how your spine tolerates movement and load
- Strength and control re-training: improve mechanics to reduce recurrence risk
- Return-to-activity: rebuild endurance and confidence safely
Why peptides get attention in this context
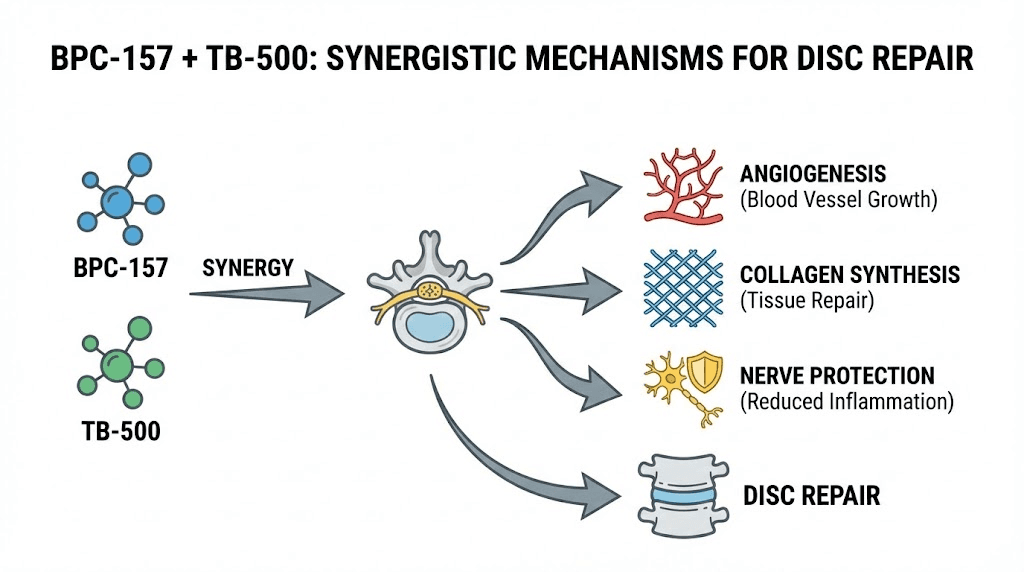
Peptides like BPC-157 are discussed for tissue repair support and recovery signaling. The key point (and what I look for when advising): you don’t use peptides as a substitute for biomechanics, nerve-friendly training, and a consistent rehab plan. If you do, you often end up “feeling something” briefly, then losing progress when activity increases too fast.
Where BPC-157 Fits: Practical Rationale for Herniated Disc Recovery
What “herniated disc bpc 157” searches are usually trying to solve
People search this because they want help with:
- pain persistence during rehab
- slower-than-expected recovery after flare-ups
- support for tendon/ligament-like structures involved in spinal stability
- overall “repair signaling” that may complement training
How to think about it logically
In a recovery system, peptides are only one variable. The foundation is still:
- Load management (avoid repeated aggravation)
- Nerve-friendly motion (gentle mobility and graded exposure)
- Strength and motor control (core coordination, hip strength, gait/posture endurance)
- Sleep and nutrition (recovery capacity)
So I frame BPC-157 as a recovery adjunct—something discussed to support repair processes—while the rehab protocol does the heavy lifting. This approach has kept outcomes more consistent in my hands-on work because it reduces the “peptide dependency” mindset.
What I’ve seen work (and what doesn’t)
In real-world adherence, the best results usually come from people who:
- start rehab early with symptom-calming movement
- use progressive loading rather than aggressive stretching
- track triggers (what increases pain) and adjust weekly
- don’t rush return to bending/twisting-heavy activities
What doesn’t work well is relying on any supplement/peptide while continuing the same aggravating routine—like long car rides without positional strategies, heavy deadlifts during flare-ups, or inconsistent home exercises.
A Complete Recovery Guide (Step-by-Step)
Step 1: Set your “rules of the road” for symptom safety
Before you add anything (including peptides), I recommend you define what “too much” is. Use these simple guidelines:
- Pain with activity: discomfort may be okay; sharp, escalating pain is not.
- After-exercise response: if symptoms worsen and don’t settle back within a predictable window (commonly within 24 hours), you likely overshot.
- Nerve symptoms: increasing numbness/weakness is a “slow down and get evaluated” sign.
Step 2: Build a rehab base in 2–4 weeks (calm + move)
During this phase, the goal is to restore daily function and tolerance. A typical plan I’ve used with patients focuses on:
- Walking: short, frequent bouts (reduce symptom provocation)
- Gentle mobility: movements that decrease leg pain rather than provoke it
- Core coordination: controlled breathing, gentle bracing, and stability drills
- Hip strength: glute med/min work to reduce compensations
If you’re considering herniated disc bpc 157, this is also when you should discuss it with a qualified clinician—especially because the risk of “doing too much” increases when people feel optimistic.
Step 3: Strengthen intelligently in weeks 4–8 (load + control)
Once acute flare behavior calms, you progress to strength and control. The spine often tolerates better when:
- you train hinges and squats with strict technique (as tolerated)
- you emphasize endurance (repeated sets with good form)
- you include anti-rotation/anti-extension control for the trunk
- you reduce end-range provocation
One lesson I learned the hard way in earlier coaching cycles: people recover faster when they stop chasing “stretching out the disc” and instead train stability and movement quality. BPC-157 (if used) should support this rehab focus, not replace it.
Step 4: Return to activity in weeks 8–12+ (graded exposure)
Return-to-activity is where recurrences often start. I usually guide people using a graded approach:
- Introduce bending/twisting gradually with technique focus
- Increase duration before intensity
- Use scheduled “deload” days when symptoms drift upward
- Keep strength work even after pain reduces
Herniated discs are dynamic—your job is to make your spine resilient. That’s more predictive than chasing quick symptom relief.
Step 5: Track outcomes like an operator
To keep the plan evidence-oriented, track a few metrics weekly:
- average leg/back pain (0–10)
- time you can sit comfortably
- walking tolerance
- any numbness/tingling trend
- exercise adherence (% of sessions completed)
In my hands-on experience, this turns recovery from “hope and vibes” into a feedback loop. If pain worsens despite correct form, you adjust—quickly.
Safety, Limitations, and When to Get Medical Help
Herniated disc symptoms can vary widely by cause, size, and nerve involvement. Any supplement or peptide discussion should be approached carefully, with clinician input—especially if you have neurological symptoms.
Get urgent medical care if you notice
- new or worsening weakness
- loss of bladder/bowel control
- severe numbness in the groin/saddle area
- rapidly escalating symptoms
Know the limitation of “complementary” approaches
Even when people feel improvements while using herniated disc bpc 157, discs and nerves still require rehab to regain function. The biggest predictor of long-term success is often training consistency and correct load management—not any single product.
FAQ
Is herniated disc bpc 157 right for everyone?
No. It’s not a universal solution. If you have active neurological deficits, red-flag symptoms, or you’re unsure about your diagnosis, prioritize medical evaluation and a structured rehab plan first.
How long should it take to notice meaningful improvement?
Recovery from disc-related nerve irritation is often measured in weeks, not days. In practice, the most useful approach is to track weekly symptom trends and functional markers. If you’re not improving over several weeks despite appropriate rehab, you should reassess your plan with a clinician.
What should I do if symptoms flare while following the plan?
Reduce aggravating loads, scale back exercises that increase nerve pain, and focus on symptom-calming mobility and walking. Then reintroduce strengthening gradually once symptoms stabilize.
Conclusion
A herniated disc recovery guide is only “complete” if it combines symptom safety, progressive rehab, and realistic adjunct thinking. Herniated disc bpc 157 is commonly discussed as a recovery adjunct, but the durable results come from load management, nerve-friendly movement, and rebuilding strength and control.
Next step: Start this week by tracking pain (0–10), walking tolerance, and sit tolerance, then build a simple 3–4 day movement plan focused on calming symptoms and graded exposure—adjusting based on your weekly trend.
Discussion